
Translate this page into:
Annular atrophic lichen planus with Koebner phenomenon
-
Received: ,
Accepted: ,
How to cite this article: Santhosh P, Aswathi TV, George M, Balakrishnan S, Shima K. Annular atrophic lichen planus with Koebner phenomenon. J Skin Sex Transm Dis 2022;4:134-5
Dear Editor,
Annular atrophic lichen planus (AALP) is the rarest variant of lichen planus (LP) which shares features of annular LP and atrophic LP.[1] Previously reported cases have demonstrated a reduction in elastin fibers in superficial dermis.[1-4] We report a case of AALP with Koebner phenomenon.
A 49-year-old female presented with multiple pruritic lesions over lower limbs for 2 years, which had started as small hyperpigmented lesions that gradually increased in size, and had failed to respond to topical steroids and retinoids. She had no comorbidities, systemic symptoms, or drug intake before the onset of the lesions. Examination revealed multiple, discrete, erythematous to violaceous, shiny, atrophic plaques over lower limbs, ranging from 2 × 2 cm to 6 × 6 cm, with a prominent raised thread-like border [Figure 1]. Mucosae, hair, and nails were unremarkable. Routine investigations including serology for hepatitis B and C were negative.

- Annular, shiny, atrophic plaque with raised thread-like border on the left leg.
Skin biopsy taken from the edge of the lesion showed epidermal atrophy with mild spongiosis and basal cell vacuolization, band-like infiltrate along the dermoepidermal junction composed of lymphocytes, polymorphs, few plasma cells and eosinophils, dispersed melanophages, and apoptotic keratinocytes [Figure 2a]. Verhoeff van Gieson stain showed absence of elastin fibers in the superficial dermis [Figure 2b]. A diagnosis of annular atrophic lichen planus was made.
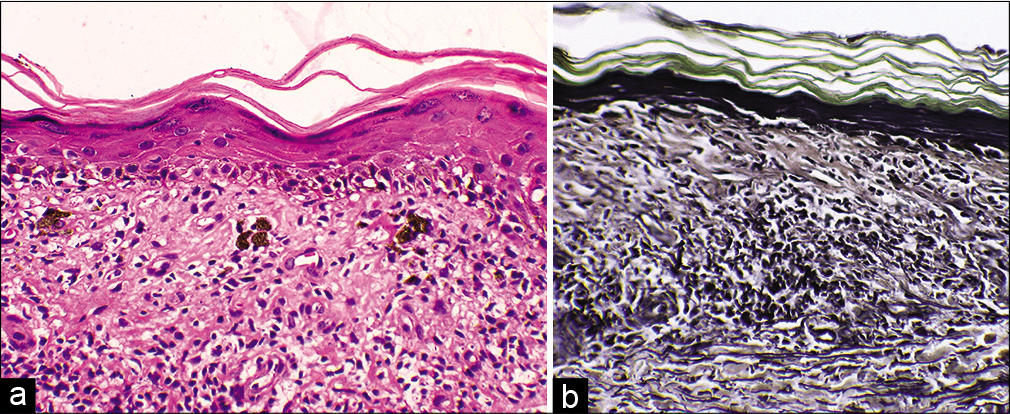
- (a) Atrophic epidermis with spongiosis and basal cell vacuolization. Dermal infiltrate of lymphocytes, polymorphs, a few plasma cells, eosinophils, melanophages, and apoptotic keratinocytes (Hematoxylin-eosin, ×400) (b) Absent elastin fibers in superficial dermis (Verhoeff van Gieson stain, ×400).
The patient reviewed after 2 weeks, having sustained minor trauma to the anterior aspect of the right leg while chopping wood. The wound had resulted in a scar of size 1 × 0.5 cm, over which he had developed an isomorphic lesion, thus demonstrating Koebner phenomenon [Figure 3]. The patient was started on 0.1% topical tacrolimus ointment. After 2 months, the pruritus subsided fully, while the lesions showed partial resolution.

- Koebner phenomenon – new lesion developing over the scar on the right leg.
Annular atrophic lichen planus is considered the rarest variant of LP with only a few published cases. It has features of both annular and atrophic LP.[1] The first case was reported in 1948, attributed to the intake of quinacrine hydrochloride, the second case in 1991, and the third in 1994. [2,3,5] AALP presents as pruritic or asymptomatic violaceous papules which expand centrifugally to form atrophic plaques with raised borders, often with a chronic course. Cases have been reported to last up to 25 years.[2] Coexistent mucosal, pilar, or nail involvement is usually absent.
Histopathology shows an atrophic epidermis with the classic features of LP, including basal liquefaction degeneration and a band-like dermal infiltrate. Previous case reports have demonstrated a scarcity of elastin fibers in the papillary dermis in AALP, varying from a partial reduction to total destruction, attributed to the elastolytic activity of the infiltrate. A similar infiltrate is evident in other types of LP as well, but elastolysis has not been reported in other LP variants. Annular LP and atrophic LP are clinical differential diagnoses of AALP, and neither have been reported to have reduced elastin fibers.[1-4] Steroid-induced cutaneous atrophy can be differentiated by prominent elastin fibers with reduced collagen bundles.[3]
AALP is relatively resistant to the conventional treatment modalities of LP, like topical steroids.[1-3] There have been a few reports of response to topical tacrolimus.[1,4] Since literature is scarce and treatment response variable, there is no current consensus regarding drug of choice or a treatment ladder.
AALP can pose a diagnostic and therapeutic challenge due to its relative rarity. Information on similar cases may help to improve the awareness regarding this entity so that effective treatment options can be formulated.
Acknowledgment
The authors express sincere gratitude to Dr. K. P. Aravindan, Medical Director, Microhealth Reference Laboratory, Kozhikode for the invaluable help in histopathology analysis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Mamatha George is on the editorial board of the Journal.
References
- Annular atrophic lichen planus. J Am Acad Dermatol. 2005;52:906-8.
- [CrossRef] [PubMed] [Google Scholar]
- An atrophic plaque in an Indian lady. Indian J Dermatol. 2014;59:211.
- [CrossRef] [PubMed] [Google Scholar]
- Generalized annular atrophic lichen planus eruption due to quinacrine hydrochloride. Arch Derm Syphilol. 1948;57:551-4.
- [Google Scholar]




