
Translate this page into:
Histopathology features in dermatitis cruris pustulosa et atrophicans: A case series
*Corresponding author: Sarita Sasidharanpillai, Department of Dermatology and Venereology, Government Medical College, Kozhikode, Kerala, India. saritasclt@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Saranya TM, Sasidharanpillai S, Govindan A. Histopathology features in dermatitis cruris pustulosa et atrophicans: A case series. J Skin Sex Transm Dis 2021;3:195-8.
Sir,
Dermatitis cruris pustulosa et atrophicans (DCPA) is a treatment-resistant, chronic, remitting, and relapsing folliculitis characterized by symmetrical follicular pustules of both legs that lead to atrophy, scarring, and alopecia.[1,2] Rarely, the lesions may involve the face, thighs, forearms, and scalp.[1,3] Majority of cases of DCPA were reported from West Africa and India.[1,3-6]
Clarke gave the name DCPA in 1952 while describing the condition among Nigerians in Lagos.[1] Different authors used different names (Nigerian shin disease, lupoid sycosis of the legs, and therapy-resistant pyogenic folliculitis of the legs) while describing the same entity.[1,3] After studying 79 cases from the Kerala state of India, Sugathan et al. suggested that the condition starts as follicular pustules, and the dermatitic changes are secondary.[1] They opined that a better terminology for the disease would be ‘folliculitis cruris pustulosa et atrophicans.[1]
Absence of constitutional symptoms such as fever and lymphadenopathy, even in those with extensive skin lesions, is a characteristic feature. Sugathan et al. proposed a clinical grading as follows.[1]
Grade 1 – Only follicular pustules seen, a few of them show perifollicular erythema
Grade 2 – Follicular pustules predominate with a significant number of infiltrated papules around broken hairs. Papules showed excoriation marks, crusting, or peripheral rim of white scales. Palpating hand could feel a wiry roughness due to the broken or irregular hairs. Alopecia may be observed, but not marked
Grade 3 – Infiltrated scaly papules predominate with a few scattered pustules at the periphery, marked alopecia, shininess, and atrophy
Grade 4 – Near-complete alopecia, skin appears atrophic, shiny, and scaly. Pustules are not seen. A few discrete scaly papules are observed at the periphery.
Sugathan et al. found a non-specific, focal round cell infiltration of the dermis and focal polymorph infiltration of the mouth of the hair follicle as the early histopathological features. They observed abscess formation of the upper part of the hair follicle in the pustular stage and atrophied rete ridges and fibrosis of dermis in the late scarring stage.[1] Harman found intercellular edema in epidermis, edema of dermis and papillae and inflammatory infiltrate composed of lymphocytes, plasma cells, eosinophils, polymorphonuclear leukocytes, histiocytes, and occasional giant cells, mainly around hair follicle, sweat ducts, and dilated blood vessels.[5]
More than a century after its initial description, the exact pathogenesis of DCPA remains unclear, and information on the histopathology features is limited.[1,3]
We report the histopathology findings of DCPA [Table 1] in five men and two women aged 21–47 years (mean age 32.9 years). The duration of the disease ranged 8–48 months (25.1 months). We classified the patients as per the grading system proposed by Sugathan et al.[3] Two patients had Grade 2, four patients had Grade 3 [Figure 1], and one patient had Grade 4 disease. None of the affected had Grade 1 disease. All except the patient with the Grade 4 disease had intense pruritus. Lesions biopsied were pustules in two patients and papules in five.
| Si. No. | Age | Sex | Duration of disease (months) | Clinical grading | Morphology of lesion biopsied | Histology finding |
|---|---|---|---|---|---|---|
| 1. | 34 | F | 8 | Grade 2 | Pustule | Hyperkeratosis, no parakeratosis, follicular plugging present, neutrophilic abscess in the stratum corneum, irregular and board-based (rete pegs fused) acanthosis, no spongiosis or exocytosis, perivascular and perifollicular inflammatory infiltrate composed of lymphocytes and plasma cells, no dermal edema |
| 2. | 46 | M | 36 | Grade 3 | Papule | Hyperkeratosis, no parakeratosis, church spire papillomatosis, no follicular plugging, no spongiosis, no exocytosis, in certain areas rete pegs joined at the lower end to form broad-based acanthosis, and perifollicular inflammatory infiltrate mainly composed of lymphocytes |
| 3. | 24 | M | 24 | Grade 3 | Papule | Hyperkeratosis, no parakeratosis, no follicular plugging, church spires papillomatosis, irregular and broad-based acanthosis, perivascular, and perifollicular inflammatory infiltrate composed of lymphocytes and plasma cells |
| 4. | 21 | M | 48 | Grade 4 | Papule | Hyperkeratosis, no parakeratosis, irregular acanthosis, blunting of rete pegs, no exocytosis, no spongiosis, no follicular plugging, perifollicular, and perivascular inflammatory infiltrate composed of lymphocytes and plasma cells |
| 5. | 23 | M | 18 | Grade 3 | Papule | Hyperkeratosis, no parakeratosis, church spires papillomatosis, irregular and broad-based acanthosis, periappendageal and perivascular infiltrate of lymphocytes and plasma cells |
| 6. | 35 | M | 12 | Grade 2 | Pustule | Folliculocentric inflammation, surrounding epidermis shows intercellular edema and inflammatory cells extending to epidermis. Inflammatory cells composed of lymphocytes, neutrophils, and eosinophils |
| 7. | 47 | F | 30 | Grade 3 | Papule | Hyperkeratosis, parakeratosis, focal spongiosis, broad-based acanthosis in certain areas, perivascular lymphohistiocytic infiltrate |

- Grade 3 dermatitis curuis pustolsa et atrophicans showing marked alopecia, dryness, papules, and scattered pustules.
We found hyperkeratosis in six patients (85.7%), irregular and broad-based acanthosis (formed by joining together of rete pegs at the lower ends) in five patients (71.4%), parakeratosis in one (14.3%), follicular plugging in one (14.3%), neutrophilic abscess in stratum corneum in one (14.3%), spongiosis in two ( 28.6%), and blunting of rete pegs in one (14.3%). We found church spire papillomatosis in three specimens (42.9%).
Six patients (85.7%) showed folliculocentric inflammation [Figure 2a]. The lone patient who did not show folliculocentric inflammation had Grade 3 disease. Neutrophilic abscess in the stratum corneum was seen in a patient with Grade 2 disease [Figure 2b]. Broad-based acanthosis was seen in all four patients with Grade 3 disease [Figure 2c] and one patient with Grade 4 disease. Three of the four patients with Grade 3 disease showed church spire papillomatosis [Figure 2d]. We found blunting of rete pegs in the patient with Grade 4 disease.
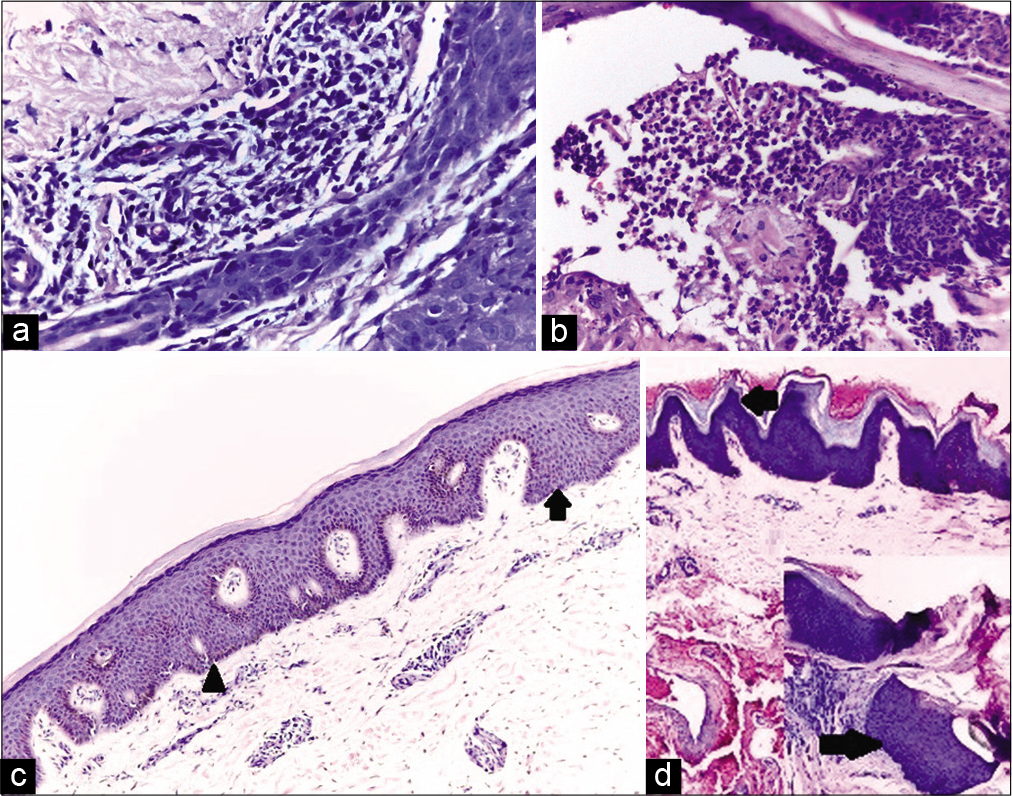
- (a) Biopsy from a patient with dermatitis curuis pustolsa et atrophicans showing inflammatory infiltrate around sweat duct, blood vessels, and hair follicle. Infiltrate extending into the epidermis with intercellular edema (H and E, ×100); (b) biopsy from a pustule of dermatitis curuis pustolsa et atrophicans showing neutrophilic abscess in stratum corneum (H and E, ×200); (c) biopsy from dermatitis curuis pustolsa et atrophicans showing broad-based acanthosis in some areas (arrow) and rete pegs beginning to fuse (arrow head) with each other in other areas (H and E, ×100); (d) biopsy from a papule of dermatitis curuis pustolsa et atrophicans showing hyperkeratosis and churchspire papillomatosis (left arrow) (H and E, ×100); inset: Another focus from the same section showing irregular and broad-based acanthosis (right arrow, H and E, ×100).
Six specimens showed perivascular and perifollicular/ periappendageal inflammation (85.7%). It was perivascular in one specimen (14.3%).
Folliculocentric inflammation and the composition of the inflammatory infiltrate, as noted by us, were consistent with the literature.[1,4-6] Giant cells were not seen in any of the specimens. This was similar to the observation of others, though Harman had mentioned a few giant cells.[1,4,5] Neutrophilic abscess and follicular plugging found in this cohort were reported earlier. [4] To the best of our knowledge, church spire papillomatosis is an undescribed feature in DCPA and could be a manifestation of chronic scratching.[7] The conditions commonly showing church spire papillomatosis on histopathology are seborrheic keratosis, acrokeratosis verruciformis of Hopf, verruca vulgaris, and acanthosis nigricans.[7] The differentiating features of seborrheic keratosis are horn cysts and pseudohorn cysts. Dermal inflammation is not a feature except in irritated and inflammatory variants.[8] Hyperkeratosis, regular acanthosis, and absence of parakeratosis and significant dermal inflammatory infiltrate characterize acrokeratosis verruciformis of Hopf.[9] Hyperkeratosis, acanthosis, hypergranulosis, large keratohyaline granules, inward turning of rete ridges at the edge of the lesions, and the presence of koilocytes differentiate verruca vulgaris from other conditions showing church spire papillomatosis.[10] Acanthosis Nigerians is characterized by hyperkeratosis and papillomatosis without any dermal inflammation.[11]
Although previous authors have described acanthosis in DCPA, we did not come across any reports highlighting its broad-based nature. Hyperkeratosis and broad-based acanthosis are considered as histopathological features of chronic dermatitis.[12] The histopathological findings of broad-based acanthosis and church spire papillomatosis could be attributed to the chronic nature of the disease (duration ranging from 8 to 48 months in this cohort) and the pruritus experienced by most of our patients (6/7, 85.7%), respectively.
We found folliculocentric inflammation and histopathology features suggestive of chronic dermatitis as the predominant finding in DCPA. Prospective studies designed to evaluate serial biopsies in different stages of the disease may give valuable information regarding the histopathology and the pathogenesis of dermatitis cruris pustulosa et atrophicans.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Sarita Sasidharanpillai is on the editorial board of the Journal.
References
- Folliculitis cruris pustulosa et atrophicans. Indian J Dermatol Venereol. 1973;39:35-40.
- [Google Scholar]
- Descriptive study on the clinical profile and demography of patients with chronic folliculitis of leg attending a tertiary referral centre. J Skin Sex Transm Dis. 2020;2:104-9.
- [CrossRef] [Google Scholar]
- Dermatitis cruris pustulosa et atrophicans. Indian J Dermatol Venereol Leprol. 2009;75:348-55.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatitis cruris pustulosa et atrophicans revisited: Our experience with 37 patients in South India. Int J Dermatol. 2009;48:1082-90.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatitis cruris pustulosa et atrophicans. Br J Dermatol. 1968;80:97-107.
- [CrossRef] [Google Scholar]
- Clinical and pathologic observations in dermatitis cruris pustulosa et atrophicans. Int J Dermatol. 1978;17:802-7.
- [CrossRef] [PubMed] [Google Scholar]
- An approach to the interpretation of skin biopsies. In: Weedon's Skin Pathology (3rd ed.). England: Chruchill Livingstone; 2010. p. :4-18. Ch. 1
- [CrossRef] [Google Scholar]
- Tumours of the epidermis. In: Weedon's Skin Pathology (3rd ed.). England: Chruchill Livingstone; 2010. p. :668-708. Ch. 31
- [CrossRef] [Google Scholar]
- Disorders of epidermal maturation and keratinisation. In: Weedon's Skin Pathology (3rd ed.). England: Chruchill Livingstone; 2010. p. :248-79. Ch. 9
- [CrossRef] [Google Scholar]
- Viral disease. In: Weedon's Skin Pathology (3rd ed.). England: Chruchill Livingstone; 2010. p. :608-31. Ch. 26
- [CrossRef] [Google Scholar]
- Miscellaneous conditions. In: Weedon's Skin Pathology (3rd ed.). England: Chruchill Livingstone; 2010. p. :502-9. Ch. 19
- [CrossRef] [Google Scholar]
- Epidermis spongiosis, acanthosis and hyperparakeratosis In: Dermatopathology (1st ed). Heidelberg: Verlag; 2008. p. :19-35. Ch. 2.
- [Google Scholar]




