
Translate this page into:
Painful skin tumor in focus: Cutaneous leiomyomas

*Corresponding author: Ankitha Adiga, Department of Dermatology, Venereology and Leprosy, Father Muller Medical College, Mangaluru, Karnataka, India. ankitha.adiga11@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Adiga A, D’Souza MJ, Bhat MR. Painful skin tumor in focus: Cutaneous leiomyomas. J Skin Sex Transm Dis. doi: 10.25259/JSSTD_64_2024
Abstract
Cutaneous leiomyomas (CLs) are rare benign tumors of smooth muscle origin, often presenting as painful papulonodules. Piloleiomyomas, a common subtype, arise from the arrector pili muscles. Although generally benign, they may be associated with hereditary conditions such as Reed syndrome, linked to fumarate hydratase gene mutations, which increase the risk of renal cell cancer. CLs are uncommon and often misdiagnosed, typically presenting in adults and requiring a skin biopsy for confirmation. Treatment options include surgical excision and cryotherapy, though managing multiple lesions can be challenging. A 57-year-old male presented with multiple asymptomatic raised lesions on his back and arms, present for over 30 years. Recently, the lesions had become painful and had increased in size and number. Physical examination revealed multiple firm, tender papulonodular lesions. An excisional biopsy confirmed the diagnosis of leiomyoma cutis. Further evaluation for renal abnormalities was negative. Initial cryotherapy sessions resulted in minimal reduction in lesion size and pain.
Keywords
Cutaneous leiomyoma
Dermoscopy
Piloleiomyoma
Reed syndrome

INTRODUCTION
The skin is the second most common site for leiomyomas after the uterus, comprising approximately 5% of all cases.[1] Cutaneous leiomyomas (CLs) are rare, often overlooked, and frequently misdiagnosed benign tumors with occasional potential for malignancy.[2] These benign smooth muscle tumors are categorized into three distinct subtypes: Piloleiomyoma, angioleiomyoma, and genital leiomyoma. Piloleiomyomas, the second most common subtype after angioleiomyomas, arise from the arrector pili muscles of the pilosebaceous unit and typically manifest as painful solitary or multiple papulonodules.[3] While the malignant transformation of CLs is rare, they can be associated with renal cell carcinoma and uterine leiomyomas in females, particularly in cases of hereditary leiomyomatosis and renal cell carcinoma, also known as Reed syndrome.[4]
CASE REPORT
We report a 57-year-old male who presented to our skin outpatient department with complaints of asymptomatic multiple raised lesions over the back and arms for the past 30 years. Recently, over the past 6 months, the lesions became painful when exposed to cold and increased in both size and number. No known comorbidities or family history of similar presentations were noted.
On physical examination, multiple tan-brown papules and nodules were noted over the shoulders, arms, and trunk. They were tender and firm in consistency, with sizes ranging from 0.5 cm to 2 cm in diameter [Figure 1]. No regional lymphadenopathy were observed.
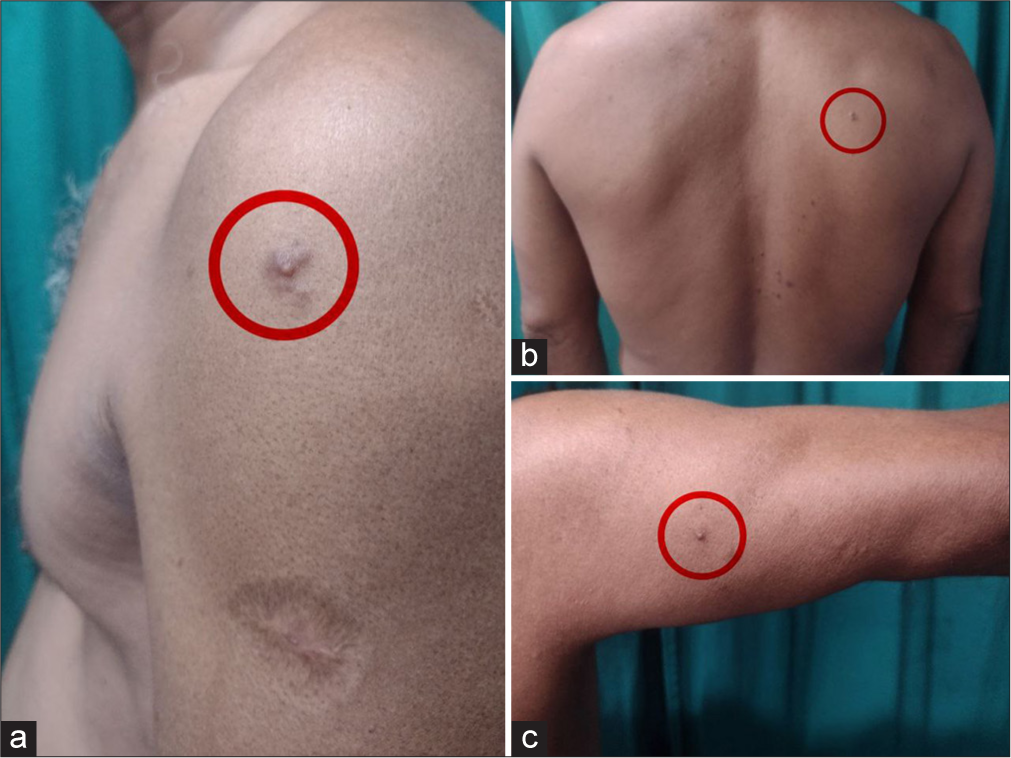
- Multiple firm papulonodular lesions noted over the (a): left shoulder; (b): back; and (c): right arm (encircled in red).
Dermoscopy of a papule showed pinkish-brown pigmented network with regular meshes and multiple white clods. The network was regularly distributed and gradually faded into the surrounding skin. No vascular changes were observed [Figure 2].
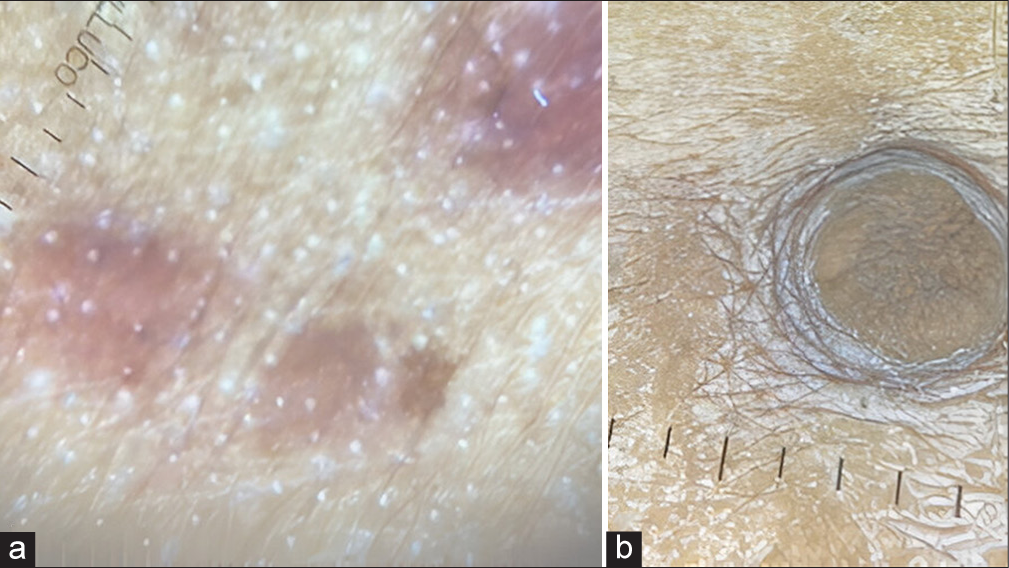
- (a): Dermoscopy shows a delicate pinkish-brown pigmented network with regular meshes and white clods (IDS 1100, Polarized light, 10X); (b): Central reticular network (IDS 1100; Non polarized light, 10X). IDS: International Dermoscopy Society.
The most prominent nodules, one from the back and one from the arm were excised for biopsy. The differential diagnosis included leiomyoma cutis and dermatofibroma. Histopathological examination of both specimens revealed well-circumscribed benign tumors in the dermis, composed of spindle cells arranged in intersecting and interlacing fascicles. These spindle cells showed bland, cigar-shaped nuclei and a moderate amount of eosinophilic cytoplasm. Focal areas of hyalinization were noted [Figure 3]. Special staining with Masson’s trichrome highlighted muscle fibers in red and collagen in blue [Figure 4]. The findings were consistent with the diagnosis of leiomyoma cutis. He was further evaluated with ultrasonography of the abdomen, and was found to be negative for any renal pathology. The patient underwent a single session of liquid nitrogen cryotherapy, consisting of three 10-s freeze-thaw cycles with a 1 mm margin. After 3 weeks, he reported a minimal reduction in lesion size and pain. He is yet to follow-up for further treatment sessions.
![(a): Epidermis appears to be normal. Focal areas of hyalinization with spindle cells (black arrow) noted at the dermis [hematoxylin and eosin (H&E, 10X)]; (b): Dermis shows smooth muscle cells with cigar-shaped nuclei and eosinophilic cytoplasm admixed with collagen bundles (H&E, 40X).](/content/102/2025/0/1/img/JSSTD-64-2024-g003.png)
- (a): Epidermis appears to be normal. Focal areas of hyalinization with spindle cells (black arrow) noted at the dermis [hematoxylin and eosin (H&E, 10X)]; (b): Dermis shows smooth muscle cells with cigar-shaped nuclei and eosinophilic cytoplasm admixed with collagen bundles (H&E, 40X).
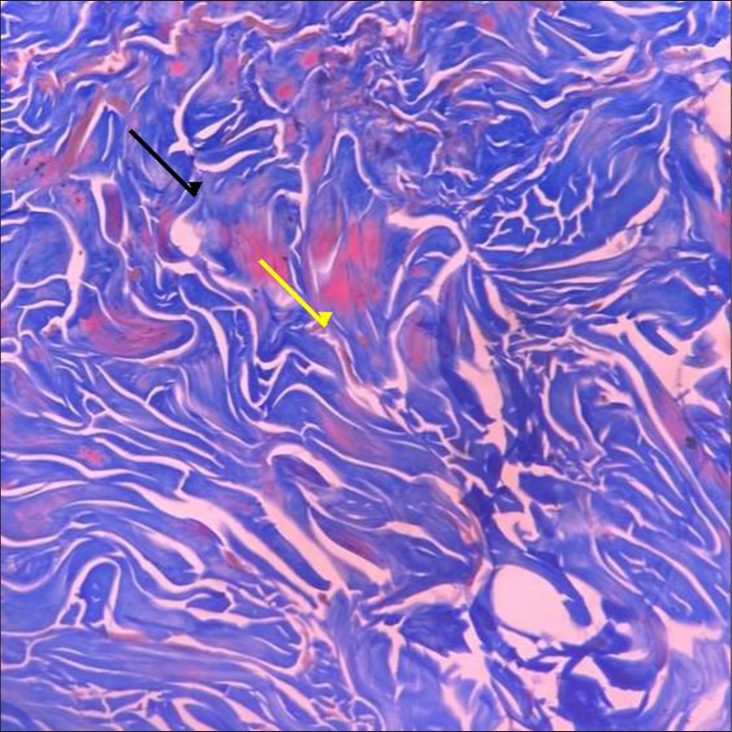
- Masson’s trichrome stain, 40X, highlighting collagen in blue (black arrow) and muscle fibers in red (yellow arrow).
DISCUSSION
CLs can appear at various locations on the skin. As in our case, they are more common in adults, typically emerging during the fifth and sixth decades of life.[3] These lesions can be either hereditary or sporadic. They are rare and challenging to diagnose and treat, often mimicking other painful, solid tumors such as dermatofibromas, angiolipomas, and neuromas. While clinical suspicion may arise, a skin biopsy is essential to confirm the diagnosis.
Multiple piloleiomyomas are commonly inherited in an autosomal-dominant manner with varying degrees of expression due to germline mutations in the fumarate hydratase gene.[5] However, they can also arise spontaneously. Hereditary cases are associated with an increased risk of renal cell cancer, necessitating careful monitoring. In our patient, there was no family history of similar lesions. He was evaluated for associated renal conditions and advised to return for annual follow-ups.
Piloleiomyomas can be either asymptomatic or painful, with discomfort reported by 50–72% of patients. The pain may result from direct pressure on skin nerves or muscle contractions mediated by α-adrenergic receptors. While solitary lesions are typically managed through surgical removal, treating multiple, widespread lesions is more challenging. Available treatments include calcium channel blockers, α-adrenergic blockers, anticonvulsants, serotonin reuptake inhibitors, and topical treatments such as 9% hyoscine hydrobromide and hyoscine butyl bromide.[6] Ongoing monitoring is necessary as these tumors can grow and compress nearby structures.
CONCLUSION
CLs, although rare, are significant due to their potential association with hereditary conditions and malignancy. Early recognition and accurate diagnosis through clinical evaluation and histopathological confirmation are essential. This case highlights the importance of comprehensive evaluation and individualized treatment strategies, emphasizing the need for ongoing follow-up to address potential complications and improve patient quality of life.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Leiomyoma cutis: A clinicopathological series of 37 cases. Indian J Dermatol. 2010;55:337-41.
- [CrossRef] [PubMed] [Google Scholar]
- A case of solitary cutaneous leiomyoma on the shoulder, mimicking a keloid: Case presentation. J Med Sci. 2020;6:34-5.
- [CrossRef] [Google Scholar]
- Cutaneous leiomyoma in a child: A case report. Oncol Lett. 2013;5:1163-4.
- [CrossRef] [PubMed] [Google Scholar]
- Leiomyoma cutis: A focused review on presentation, management, and association with malignancy. Am J Clin Dermatol. 2015;16:35-46.
- [CrossRef] [PubMed] [Google Scholar]
- A retrospective review of 48 individuals, including 12 families, molecularly diagnosed with hereditary leiomyomatosis and renal cell cancer (HLRCC) Fam Cancer. 2018;17:615-20.
- [CrossRef] [PubMed] [Google Scholar]
- Successful treatment of multiple cutaneous leiomyomas with carbon dioxide laser ablation. Postepy Dermatol Alergol. 2015;32:480-2.
- [CrossRef] [PubMed] [Google Scholar]




