
Translate this page into:
Semicircular lipoatrophy – An overlooked entity
*Corresponding author: Vinayak Viswanath, Department of Dermatology and Venereology, Government Medical College, Thiruvananthapuram, Kerala, India. vinayakviswanath21@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Viswanath V, Jully M, Duyu T, Thomas SB. Semicircular lipoatrophy – An overlooked entity. J Skin Sex Transm Dis 2024;6:87-9. doi: 10.25259/JSSTD_4_2023.
Dear Editor,
Semicircular lipoatrophy (SCL) or Lipoatrophia semicircularis, a localized lipodystrophy affecting the subcutaneous fat, is characterized by horizontal, semicircular band-like depressions that usually involve the lower limbs bilaterally.[1] The overlying skin remains clinically normal.[2]
Underlying pathogenesis is thought to be repeated microtrauma, usually in the workplace, which often goes unnoticed by patients.[1,3] Avoidance of the precipitating trauma ensures prompt and spontaneous resolution.[3]
Here, we report a woman who developed unilateral SCL.
A 50-year-old female teacher with a history of hypertension presented with an asymptomatic, semicircular depression on her right thigh of 1.5-years duration. She denied any preceding local inflammation, trauma, injections, constitutional symptoms, or symptoms suggestive of internal organ involvement.
Clinical examination revealed a skin-colored, horizontal, semicircular depression of 10 × 3 cm size on the upper, and anterolateral aspect of the right thigh without any discoloration, inflammation, or induration [Figure 1a]. Complete hemogram and urine microscopy analysis did not reveal any abnormalities. High-frequency ultrasound (HFUS) examination of the lesion revealed normal epidermis and dermis, while subcutaneous fat showed a focal area of reduced thickness with a 6.3 mm decrease in comparison to the left thigh at the same level [Figure 1b]. The subcutaneous fat and septa, muscle layer, and intermuscular septum showed normal echogenicity without any evidence of edema or increased vascularity on color Doppler.
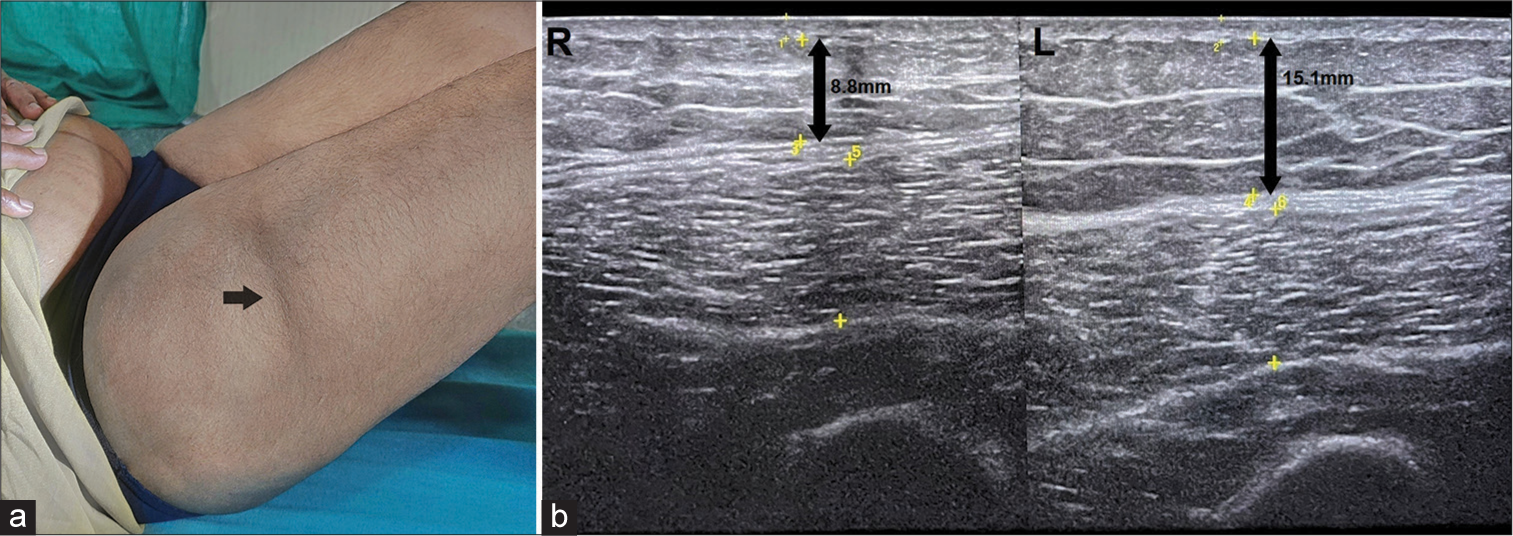
- An ill-defined, horizontal, and band like depression on the anterolateral aspect of right thigh (black arrow); (b): Ultrasound image of thighs showing reduced thickness of subcutaneous fat layer (double headed black arrows) on the right side when compared to the left.
On further questioning, the patient confirmed a long-standing habit of leaning over wooden desk during teaching, probably more on the right side, which explained the unilateral manifestation. Histopathology showed mild epidermal atrophy and slightly increased dermal collagen, with diminutive fat lobules composed of small to medium-sized lipocytes in subcutis without any dermal or subcutaneous inflammation [Figures 2a and b].
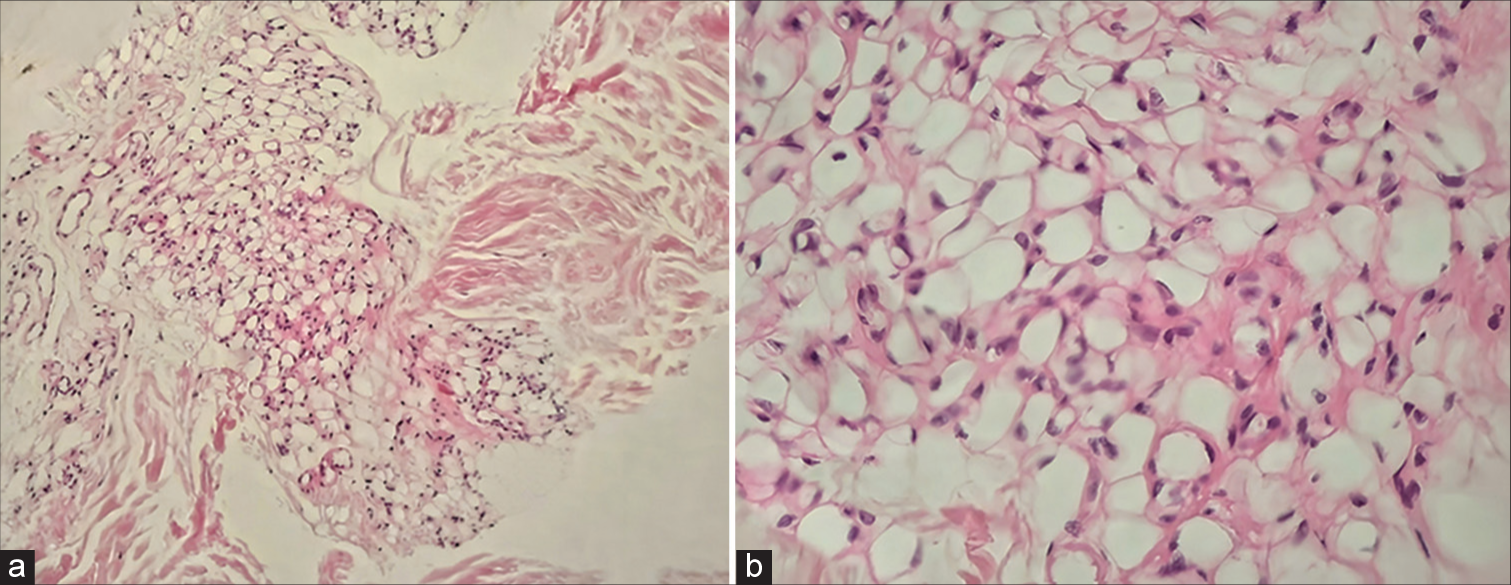
- Histopathology showing diminutive fat lobules in subcutis (H&E, ×100); (b): Higher magnification showing fat lobules composed of small to medium-sized lipocytes and devoid of inflammatory cells (H&E, ×400).
The history of repeated microtrauma, decreased subcutaneous fat on ultrasonography and lack of inflammatory changes on histopathology favored the diagnosis of semicircular lipoatrophy. Once the patient took a conscious effort and changed her posture while teaching (avoided leaning on the wooden desk), the lesion showed improvement and resolved within a few months.
SCL has been defined as bilaterally, symmetrical or unilateral, and horizontal band-like lesions involving the anterior or anterolateral surface of thighs. As per the diagnostic criteria proposed by Bru-Gorraiz et al., the length of the lesions is at least 3 times their width.[3]
The condition shows a female predilection; most of the affected are around the age of 40 years.[1,3] The female preponderance is attributed to the higher proportion of subcutaneous fat in females (in comparison to males). Moreover, females are more likely to seek medical advice for cosmetic concerns.[1]
Repetitive microtrauma is said to be the precipitating event, which in turn leads to alterations in adipocyte differentiation.[4] Pressure against the sharp edges of desks are often implicated in thigh lesions.[1,3] This theory is supported by the observation of uniformity of the distance between the floor and the horizontal indentations on the lower limbs, despite differences in height among affected patients.[1]
Peters and Winkelmann described two distinct histopathological patterns of SCL.[4] They include the “inflammatory” type, with perivascular and periseptal lymphocytic inflammation, normal lipocytes and vasculature, and the “involutional” type, with diminutive lobules composed of small to medium-sized lipocytes, abundant hyaline material, and prominent vessels, but without inflammatory cells.[4] The authors also reported a “normal” case without any significant histopathological changes in the subcutis.[4]
HFUS is a useful and non-invasive tool in the diagnosis of SCL. Reduced subcutaneous tissue thickness with prominent septa in the absence of any edema, increased vascularity, or evidence of dermal changes on HFUS indicates SCL.[5] The hyperechoic and prominent septa seen in SCL may correspond to septal fibrosis on histology.[5] HFUS is also used to monitor the resolution of atrophy after avoidance of the identified cause.[5]
In the majority of cases, multiple external influences can contribute to the development of SCL and the lesions usually resolve within 4 months of cessation of exposure to the workplace environment that precipitated the lesion.[1,3]
Individual actions recommended to prevent or attain resolution of SCL include avoiding leaning the body against the edges of furniture, adjusting chair height to prevent thighs from coming into contact with desks, and resting feet on the floor or footrest.[3]
It is important to differentiate SCL which has a favorable outcome, from other persistent conditions that show an apparent reduction in subcutaneous tissue thickness.[3]
A thorough history, including probing for any history of repeated trauma, aids in the diagnosis and management of this condition.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Lipoatrophy semicircularis induced by trauma. Clin Exp Dermatol;. ;26:269-71.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=11990 [Last accessed on 2023 Feb 23]
- Lipoatrophia semicircularis: Clinical study and follow-up of 76 cases in Madrid, Spain. Classification proposal. Actas Dermosifiliogr. 2022;113:15-21.
- [CrossRef] [PubMed] [Google Scholar]
- The histopathology of localized lipoatrophy. Br J Dermatol. 1986;114:27-36.
- [CrossRef] [PubMed] [Google Scholar]
- Semi-circular depression on the leg diagnosed by high-frequency ultrasound: A quiz. Acta Derm Venereol. 2021;101:adv00524.
- [CrossRef] [PubMed] [Google Scholar]




