
Translate this page into:
Tripe palms with acanthosis nigricans: Unusual cutaneous markers of poorly differentiated hepatocellular carcinoma
*Corresponding author: Betsy Ambooken, Department of Dermatology, Government Medical College, Thrissur, Kerala, India. joebetsy123@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ambooken B, Deepthi P, Mathew A, Asokan N. Tripe palms with acanthosis nigricans: Unusual cutaneous markers of poorly differentiated hepatocellular carcinoma. J Skin Sex Transm Dis 2022;4:143-5.
Dear Editor,
Paraneoplastic dermatoses are cutaneous reaction patterns to internal neoplasms which can closely resemble a number of dermatoses. These may represent the first sign of an underlying neoplasm or the earliest symptom of relapse of a previous cancer.[1]
Tripe palms is a rare cutaneous syndrome, in which the palms develop velvety thickening and rugosity that creates an exaggeration or distortion of dermatoglyphics resembling boiled tripe. In more than 90% of patients, tripe palms are associated with malignancy, predominantly pulmonary and gastric carcinomas.[2] Tripe palms occur alone or frequently in conjunction with acanthosis nigricans (AN).[2] Addisonian pigmentation can occur as a paraneoplastic manifestation which manifests as diffuse brown-black pigmentation accentuated over sun exposed skin, flexures, and palmar creases often associated with pigmentation of buccal mucosa and nails.[3]
A 47-year-old male was referred to dermatology department for diffuse hyperpigmentation of face and oral mucosa. He was admitted in medicine ward for evaluation of recurrent episodes of abdominal pain, loss of appetite, and loss of weight for the past 1 year and vomiting of 2 weeks duration. There was no history of any other significant medical illness. He was not on any drugs before admission to our institution. On examination, he was emaciated and pale with dry sunken eyes and loss of facial pad of fat. His blood pressure was 90/60 mm of mercury. He had diffuse hyperpigmentation, more marked on the face and neck with pigmentation of buccal mucosa and tongue. The skin of the dorsal aspect of hands and feet showed hyperpigmentation and thickening and had a velvety texture [Figure 1a]. Palms were hyperkeratotic with exaggerated dermatoglyphic ridges [Figure 1b]. Systemic examination revealed non tender, firm, smooth hepatomegaly with ascites. A clinical diagnosis of tripe palms with acral AN and diffuse hyperpigmentation was made.
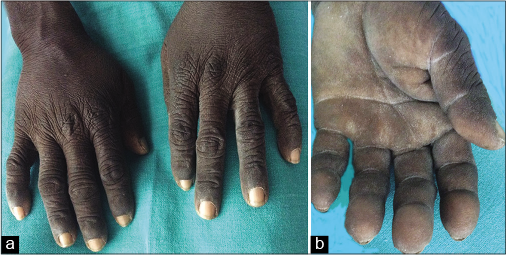
- (a) Velvety appearance of acanthosis nigricans involving the dorsum of hands in a patient with hepatocellular carcinoma. (b) Palm showing hyperkeratosis with exaggerated dermatoglyphic ridges in a patient with hepatocellular carcinoma.
Laboratory investigations revealed anemia (hemoglobin: 10.5 g/dl) and normal total and differential counts. Peripheral smear analysis showed normocytic normochromic anemia. Fasting blood sugar was 92 mg/dl. Liver function tests revealed elevated liver enzymes {serum glutamic oxaloacetic transaminase: 224 IU/L, serum glutamic pyruvic transaminase: 142 IU/L} and international normalized ratio (INR 1.68). He had hyponatremia (serum sodium: 129 mEq/l). Serum potassium (3.6 mEq/l) and cortisol (21.54 mcg/dl) levels were normal. Serum adrenocorticotrophic hormone level could not be tested due to financial constraints. X-ray chest and serum Vitamin B12 levels were normal. Renal function tests were normal. Serology for human immunodeficiency virus and hepatitis B and C infections was negative. Cytology analysis of ascitic fluid did not show malignant cells. Ultrasonogram of abdomen revealed mild hepatomegaly with heterogenous echotexture. Contrast-enhanced computerized tomogragraphy of abdomen showed inhomogenous hepatic parenchymal enhancement [Figure 2] and diffuse ascites. Upper gastrointestinal endoscopy was normal. Fine-needle aspiration cytology from liver was suggestive of poorly differentiated hepatocellular carcinoma [Figure 3].

- Contrast-enhanced computerized tomography abdomen showing inhomogenous hepatic parenchymal enhancement.

- Fine-needle aspiration cytology of liver showing poorly differentiated malignant hepatocytes (Papanicolaou’s stain, ×400).
Our patient had tripe palms with AN mostly limited to dorsum of hands and feet. Tripe palms with predominantly acral AN in poorly differentiated hepatocellular carcinoma have been rarely reported. There is one previous report of tripe palms associated with AN and Leser-Trelat sign in hepatic hemangiopericytoma.[4] The more frequent internal malignancies associated with tripe palms are those of gastrointestinal tract, lungs, bladder, breast, female genital tract, ovary, and kidneys.[5] The cause of tripe palms is not clearly understood, but is thought to be related to the secretion of growth factors such as transforming growth factor α, structurally related to epidermal growth factor, which increases the mitotic rate and consequently causes epidermal hyperplasia.[6] In classical malignant AN, there is abrupt onset of AN involving neck and flexures with mucosal involvement. In our case, AN was predominantly acral and was not associated with mucosal papillomatous lesions. In addition, our patient also had diffuse hyperpigmentation of skin mainly over the face and neck which lacked other features of AN such as thickening or velvety texture. Although advanced liver disease and profound cachexia too can cause diffuse hyperpigmentation, the accentuation of pigmentation over sun exposed areas and flexures with presence of pigmentation on the tongue and buccal mucosa favored the possibility of paraneoplastic Addisonian pigmentation. The Addisonian pigmentation noted could possibly be due to the melanogenic action of melanotrophic hormones such as alpha melanocyte stimulating hormone or ectopic ACTH secreted by the tumor cells.[3] Unfortunately further evaluation of the patient was not possible as he succumbed to his illness within a few days of admission.
Our case highlights the unusual coexistence of tripe palms, predominantly acral AN, and diffuse pigmentation (possibly Addisonian) in hepatocellular carcinoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Betsy Ambooken and Dr. Asokan N are on the editorial board of the Journal.
References
- Paraneoplastic addisonian pigmentation and acquired ichthyosis as presenting features of multiple myeloma. J Coll Physicians Surg Pak. 2011;21:40-2.
- [Google Scholar]
- Acanthosis nigricans, tripe palms and the sign of leser-trelat in a patient with a benign hepatic neoplasia. J Eur Acad Dermatol Venereol. 2007;21:846-8.
- [CrossRef] [PubMed] [Google Scholar]
- Tripe palms associated with malignant acanthosis nigricans in a patient with gastric adenocarcinoma: A case report and review of the literature. Dermatol Online J. 2012;18:15.
- [Google Scholar]
- Activation of epidermal growth factor receptor/ERK signaling correlates with suppressed differentiation in malignant acanthosis nigricans. J Invest Dermatol. 2002;118:891-3.
- [CrossRef] [PubMed] [Google Scholar]




